OSCE and Learning Points
A)OSCE Pre-Final Examination:-
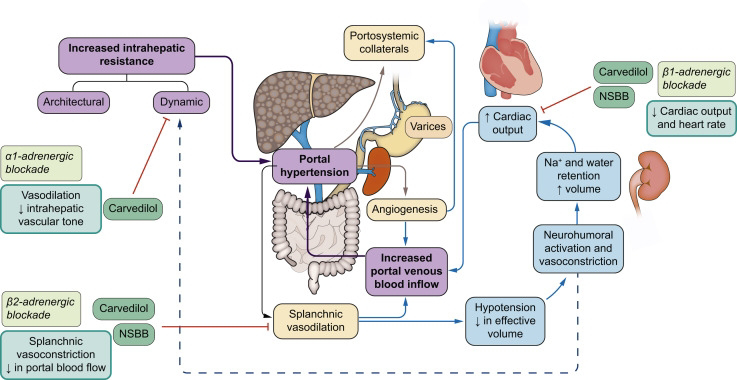
1.Mechanism of Ascites:-



2.Medical management of Ascite:-

*Role of Beta-blockerd in Ascites:-
3.Shunt treatment for Ascites:-
Peritoneovenous shunt placement is performed as a long- term treatment for chronic refractory ascites. The shunt used most commonly is the Denver shunt, comprised of two silastic tubes connected by a compressible pump.

**Indications:-
PVS is effective in the drainage of the peritoneal fluid in patients with chronic refractory ascites. The most common indication for insertion of PVS is medically intractable ascites secondary to chronic liver diseases. Conditions that result in chronic ascites that is unresponsive to medical therapy are best treated with PVS. These include acute and chronic liver diseases like cirrhosis, malignant ascites due to malignant tumors of the breast, ovary, or colon, chylous ascites, congestive heart failure, chronic kidney disease (CKD), and portal vein thrombosis.PVS is indicated under the following conditions:
->Malignant or cirrhotic ascites unresponsive to medical treatment and large volume paracentesis
->Chylous ascites
->The patient is unresponsive to diuretics.
->The patient is not a candidate for liver transplantation.
->The patient is not a candidate for serial therapeutic paracentesis due to extensive abdominal surgical scars.
->The patient has a life expectancy of more than three months.
->The patient has no contraindication to PVS.
->Non-availability of physicians to perform serial therapeutic paracentesis.
Technique:-
The most commonly used PVS is the Denver shunt, which a modified version of the original design. After the patient is prepped and draped, an all-purpose drainage (APD) catheter is inserted at the upper abdominal region to drain the ascitic fluid. It is then replaced with the peritoneal end of the shunt after priming it with warmed saline. It is inserted between the right hepatic lobe and the ribs. The second incision is made on the lower rib cage for the placement of the compressible pump. It must be placed against a firm, stable rib for effective compression. The third incision is made at the venous access site. Using a long metallic tunneler, the shunt is traversed towards the neck, ideally subcutaneously; however, it can also be placed percutaneously.
The venous end of the shunt is inserted into the superior vena cava via the internal jugular veins or the subclavian veins under fluoroscopic guidance until the catheter tip ends in the proximal right atrium. A one-way pressure-sensitive valve is attached to prevent the backflow of blood from the venous end of the shunt.
4.Complications from PVS:-
Common and include:-
Peritoneal Infection,
Variceal Bleeding,
Superior Vena Cava Thrombosis,
Pulmonary Edema,
Disseminated Intravascular Coagulation (DIC), Scar Tissue Formation,
Shunt fracture,
Occlusion,
Displacement or Leakage,
Pneumothorax, and Pneumoperitoneum.
The most common complication of PVS is Shunt Occlusion, with only 18.6% of shunts remaining patent at two years, according to a study.
About 9% of the patients report with disseminated intravascular coagulation (DIC) after shunt insertion.This condition may be due to the presence of activating factors like tissue factor (TF) that initiate thrombogenesis. Thrombosis of the shunt is a rare occurrence and mainly involves the tip of the venous end of the shunt.
Staphylococcal and gram-negative organisms can result in perioperative infections, which may progress to bacterial peritonitis or sepsis.
B)Learning Points in Long Case:-
1. Indications of dialysis
2. How to approach a patient, Take detailed history and link the past illness history with the present complaints.
3. About Rat Poisoning
4.How to differentiate Joint pain, muscle pain and bone pain.
5. Learnt about Gout and Rheumatoid arthritis.

Comments
Post a Comment